COD 199 - Two PAVMs, Two Patterns
PAVMs are usually easy to diagnose with specific points that need to be mentioned in the report.
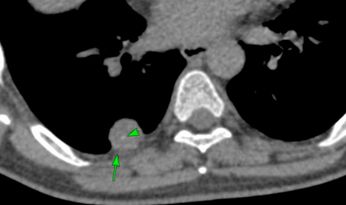
Case:
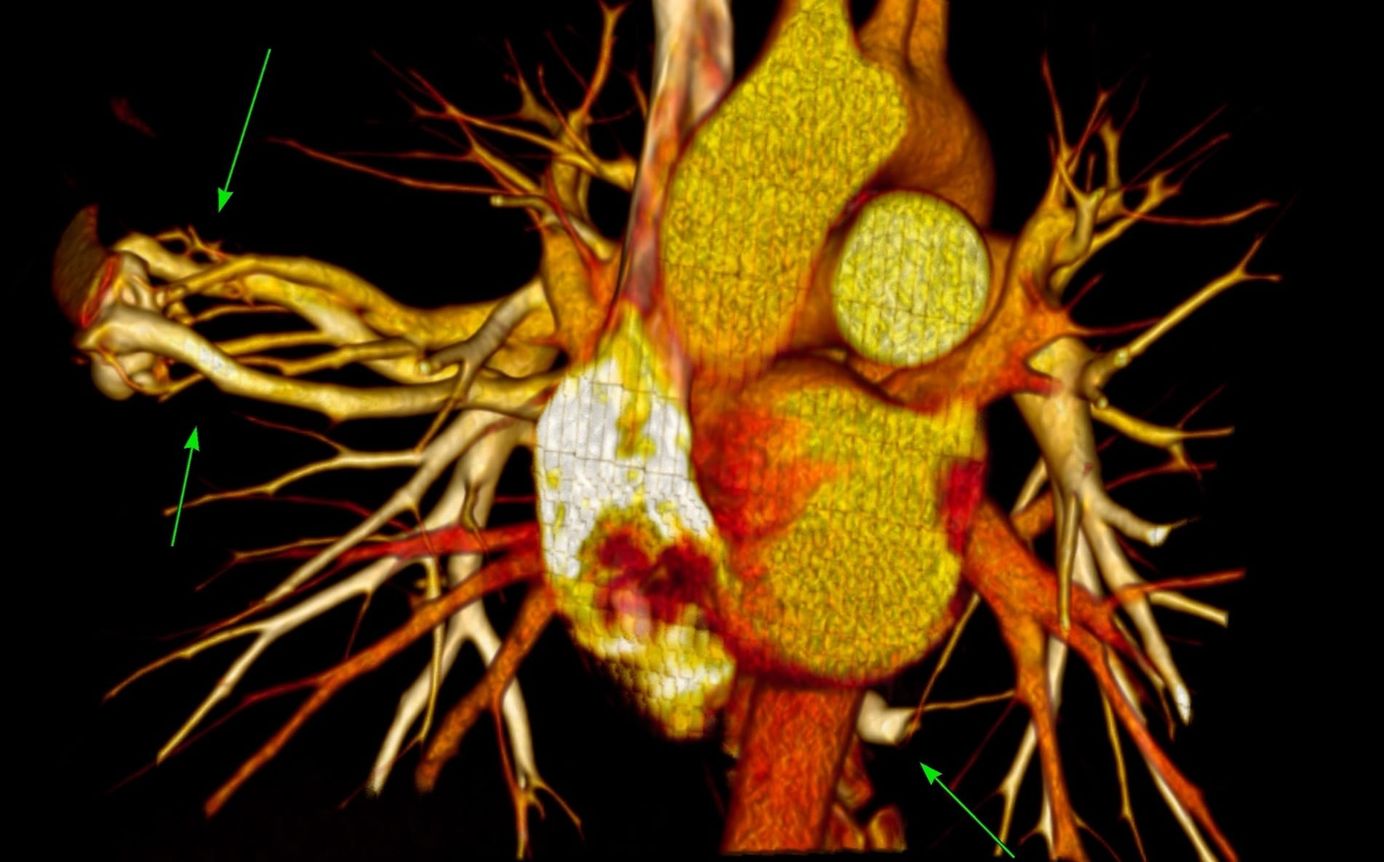
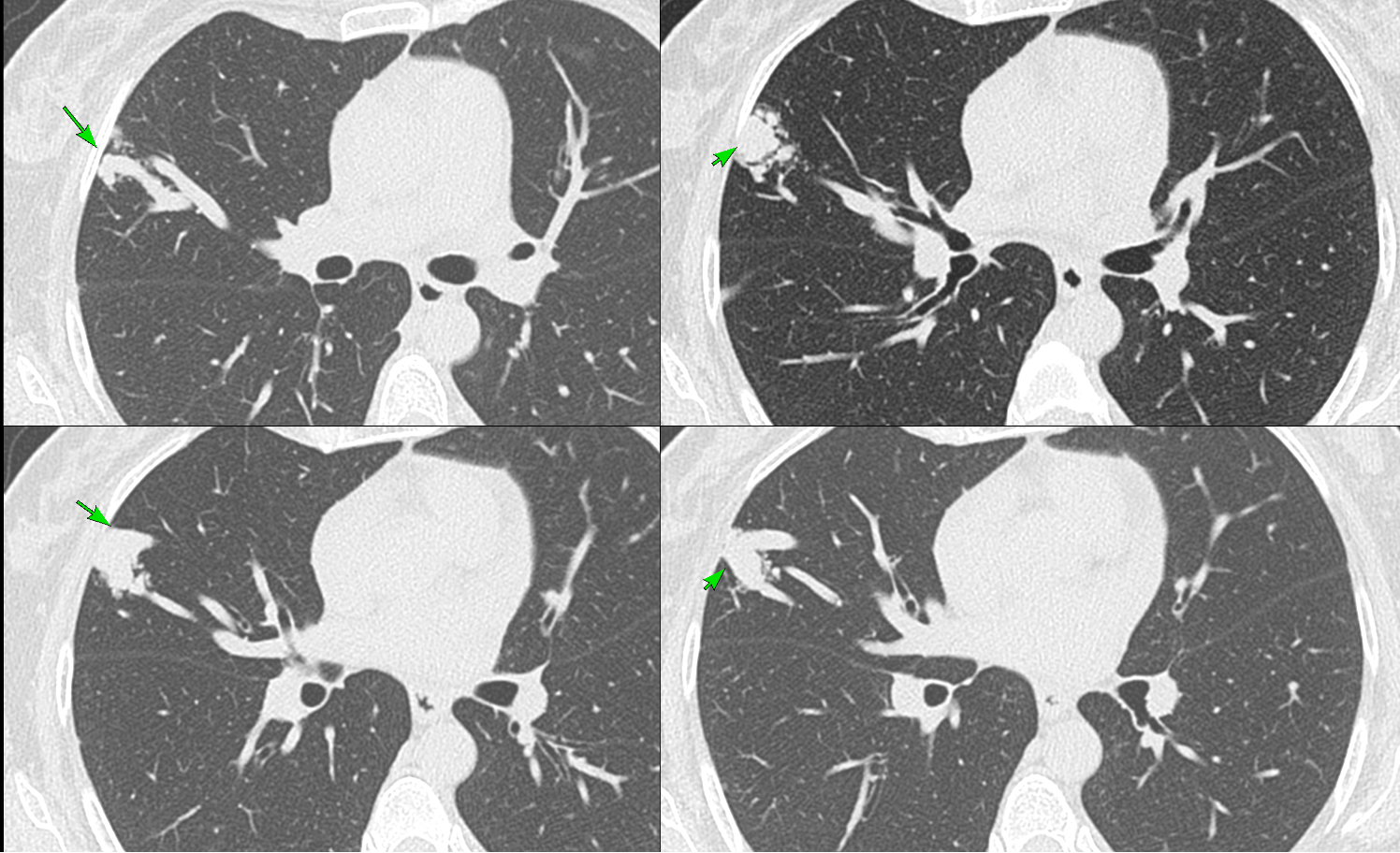
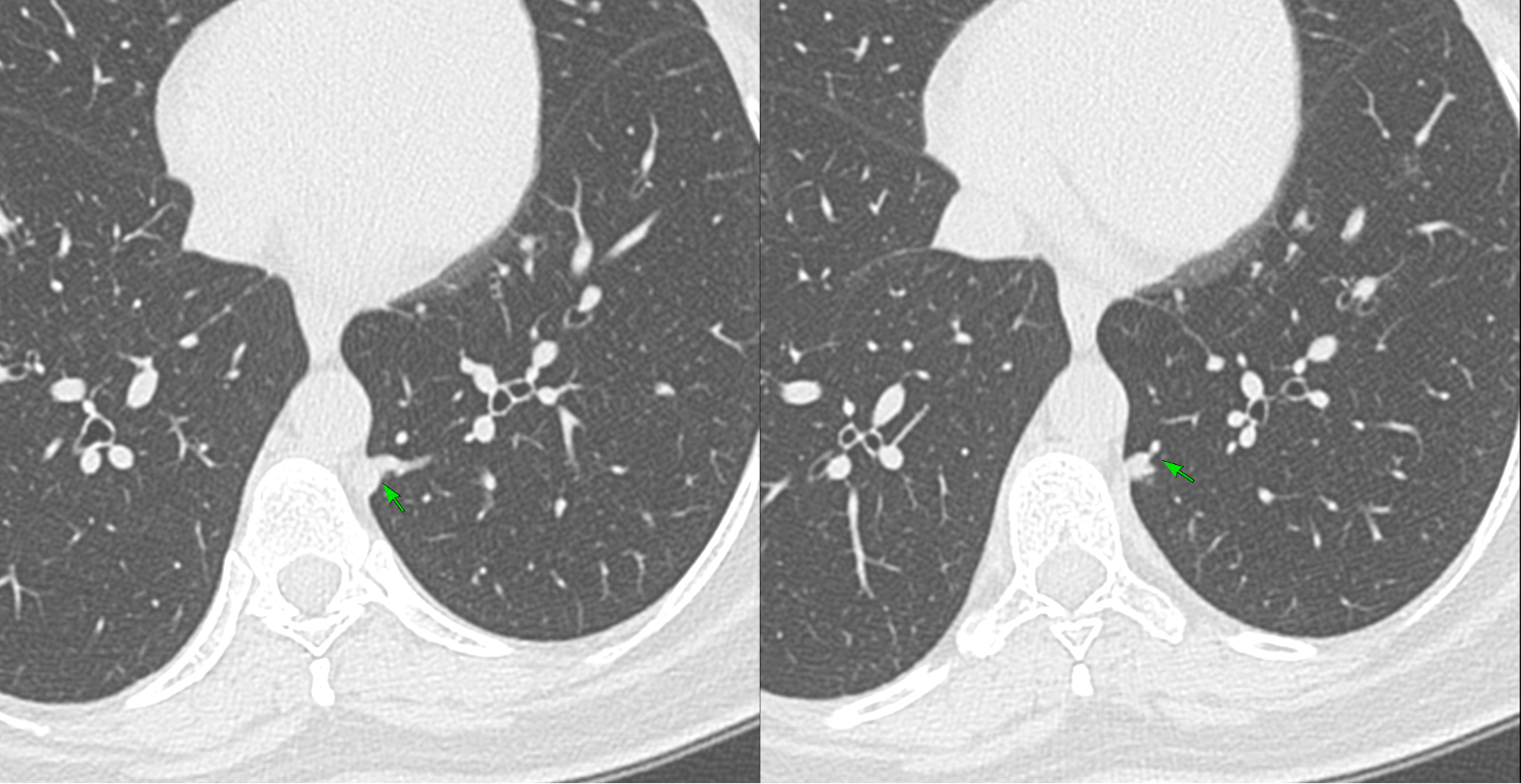
43-years old lady who had had one episode of peri-AVM bleeding presented for workup. She was known to have PAVMs since 2019.
The video discusses the following
- Classification of PAVMs — simple, complex, diffuse, telangiectatic
- The old "3 mm rule" is obsolete — the new CIRSE embolization threshold is a feeder diameter of 2.0 mm, and neurologic events have been documented at even smaller calibres when other high-risk features are present
- Four anatomic predictors of stroke and brain abscess: feeder ≥ 2.0 mm, sac ≥ 3.5 mm, sac-to-feeder (SF) ratio ≥ 1.4, and multi-saccular morphology
- Why the SF ratio matters — a small feeder with a disproportionately large sac (PAVM 2: SF 5.27) is just as worrying as a large complex lesion
- Intra-saccular thrombus, perilesional bleeding, and systemic arterial supply — features general radiologists frequently miss
- Multiple PAVMs in one patient → independent elevation of neurologic risk; mandates HHT workup (Curaçao criteria + genetic testing)
- A practical CT reporting checklist for thoracic and general radiologists
This post is for subscribers only
SubscribeAlready have an account? Log in
{kind=link}